
HeyPenny Case Study:
Capital & Coast Department of Anaesthesia

Overview
The Capital and Coast Department of Anaesthesia (CCDOA) undertook a five-month executive-level pilot to explore whether regular leadership check-in conversations could strengthen executive visibility into team wellbeing and workplace pressures. The pilot was designed as a focused intervention to provide department leads with oversight of their senior team, validate the impact of previous wellbeing investments, and offer direct support to the executive cohort.
Twelve executive leaders participated in three 1:1 conversations with Dr. Hillary Bennett, an external organisational psychologist. To ensure best-practice delivery and to mitigate the significant time pressures faced by senior clinicians, an external facilitator was used for this initial stage. Insights were captured using the HeyPenny platform, allowing core psychosocial factors (aligned to ISO 45003) to be analysed at an aggregated level.
The pilot served two purposes: to give department leadership clearer oversight of the executive team's current experience, and to validate this approach within a high-pressure healthcare setting as part of a wider multi-stage evaluation across different regions.
Context / The Challenge
CCDOA operates within a complex and demanding healthcare environment. The department is large, shift-based, and often disconnected due to differing clinical schedules. This structure makes consistent visibility across teams difficult, even at the executive level.
The nature of anaesthesia carries high responsibility, significant cognitive load, and the potential for periods of acute stress. Across Aotearoa, anaesthesia departments have faced serious wellbeing challenges, including instances of suicide within the profession. Broader systemic pressures in healthcare, including workforce shortages and retention challenges, further intensify this environment.
While Wellington Hospital had invested in wellbeing apps and initiatives previously, these solutions had not always landed well or maintained traction. Department leads Sheila and Sally were seeking a more consistent, detailed view of how work was impacting their people, where risks sat, and how best to support their people.
The pilot presented an opportunity to move beyond assumptions and gain real-time qualitative insight.
Pilot Design
The pilot ran for five months and was intentionally designed as an executive-level intervention. The twelve leaders participated in three 30-minute 1:1 check-ins facilitated by Dr Hillary Bennett, an external consultant, where conversations focused on the impact of work and explored key psychosocial factors through open discussion and self-reflection.
This approach served several purposes:
To model best-practice 1:1 conversations in a psychologically safe setting facilitated by an expert
To test the feasibility of check-ins as an intervention and data collection method
To generate rich, real-time data that gave department leads thorough oversight
To provide immediate wellbeing support for the leaders
The HeyPenny platform was used to log each conversation, with the AI Agent generating concise, anonymised, unbiased insights categorised against core psychosocial factors and marked as protective, neutral, or harmful. This allowed individual reflection while also building an aggregated executive-level view.
Department leaders Sheila and Sally were given access to the aggregated data at the half way point, giving them real-time oversight as the pilot continued. At the end of the pilot, they were also provided with an Executive Level Report that outlined the top factors along with common themes found within them.
Pilot Outcome
Platform Data

Across the pilot:
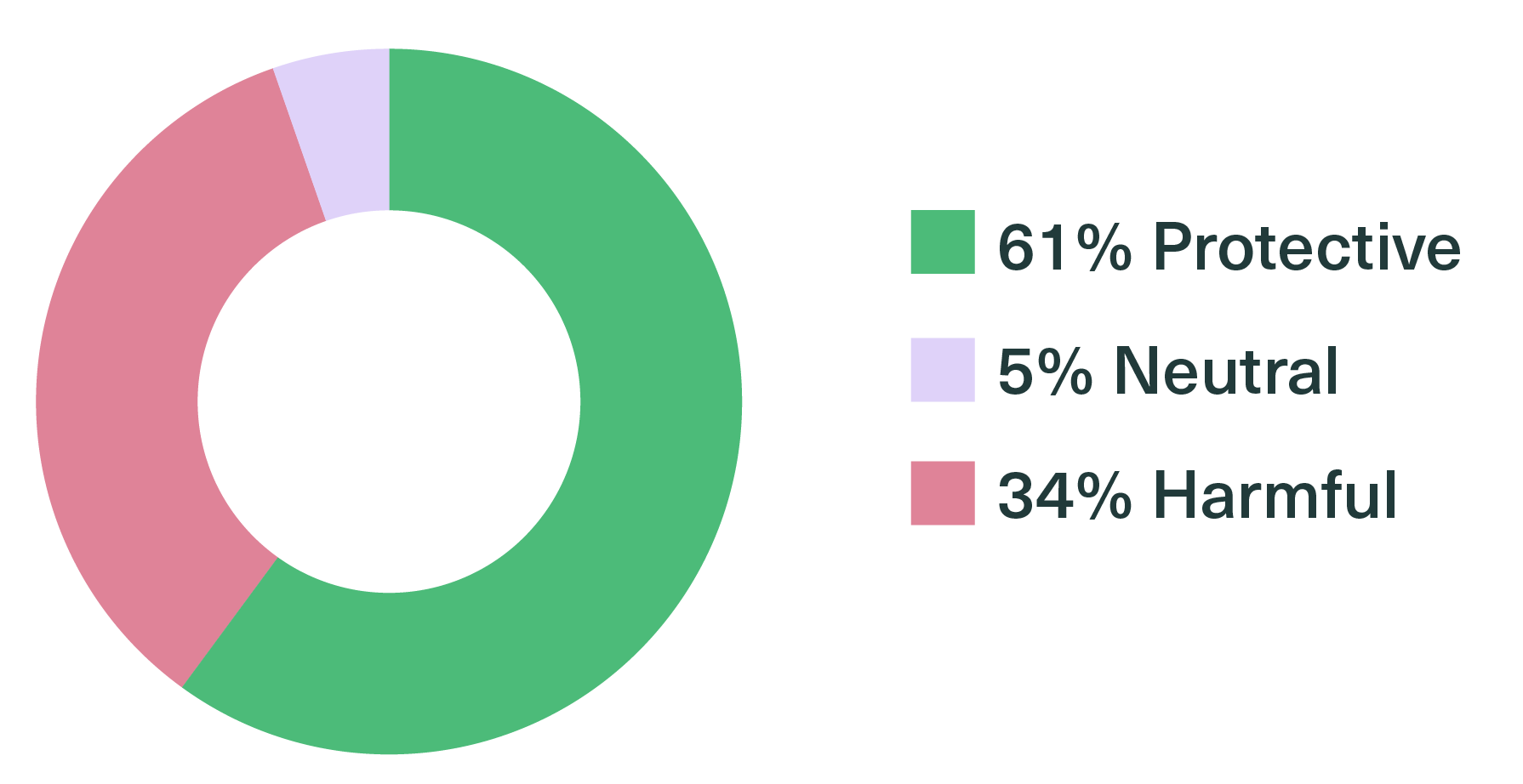
Overall insight weighting:
Observed Outcomes
Increased Visibility for Leadership
For department leads Sheila and Sally, the aggregated insights provided greater visibility across the executive cohort than had previously been possible. The aggregated qualitative and quantitative data provided greater clarity about themes, pressures, and strengths within the executive group. This confirmed that the check-in model is a powerful approach for gaining oversight into a senior team’s health.
Deeper Conversations Over Time
Conversations evolved across sessions two and three. Initial discussions focused on systems-level pressures and operational constraints. Over time, dialogue moved toward more nuanced reflections, suggesting growing trust and psychological safety.
Space for Executive Reflection
Leaders reported valuing the protected time for reflection with an external facilitator. In an environment largely focused on patient care and operational delivery, having structured space to consider their own experience was described as beneficial.
Validation of Prior Efforts
The data provided critical validation for leadership. For example, Rest & Recovery emerged as a top protective factor, confirming that previous efforts to support balance within the department were having a tangible, positive impact.
Shifting Scepticism
There was initial scepticism about whether conversations alone would make a difference, particularly given the complexity of schedules and limited overlap between team members. While logistical coordination was challenging at the outset, scheduling became easier over time, suggesting increasing willingness to participate.
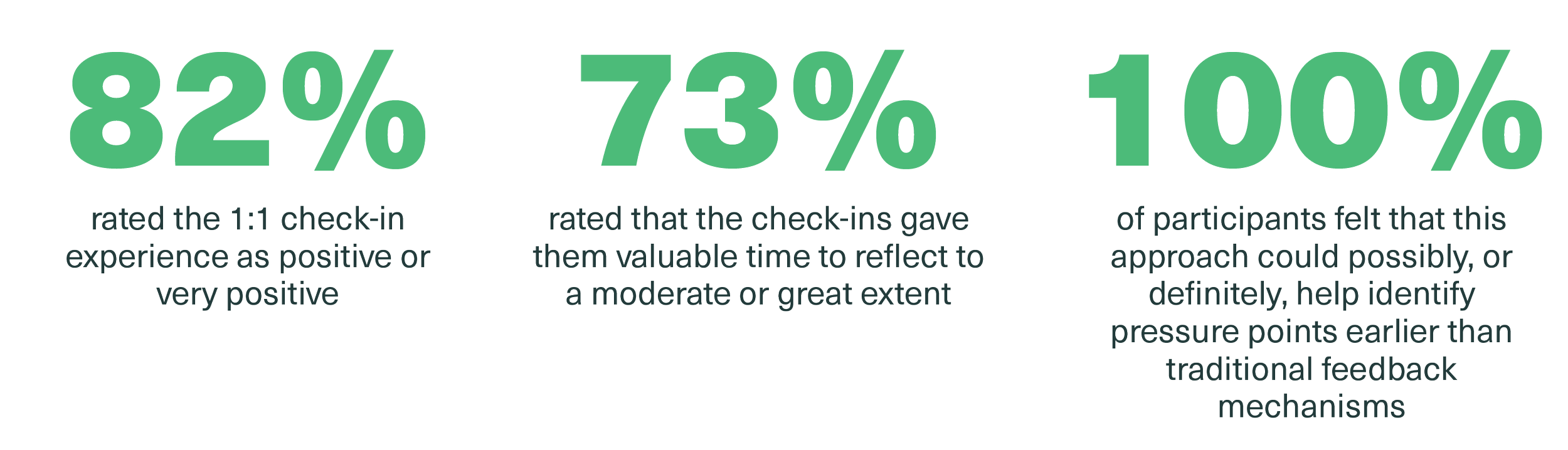
Leadership Experience
Eleven (out of 12) leaders completed a post-pilot survey which showed overall sentiment was positive:
Next Steps
This pilot successfully met its objectives as a validation phase within a healthcare setting. It proved that the HeyPenny platform can transform 1:1 check-in conversations into actionable oversight data, providing leadership with a clear way to identify pressure points early.
Following this, HeyPenny is moving into a second stage of testing with other health departments and regions around New Zealand. This next phase will transition from external facilitation to using internal leaders to hold the check-ins, specifically exploring how to balance the clear benefits of the insights with the operational realities of clinical environments.